Assoc. Prof. Ekrem GUNER, MD

Dear colleagues,
I am honored to share with you the second issue of 2025 (volume 6, issue 2) of the Grand Journal of Urology (Grand J
Urol) with the contributions of many respected researchers and authors.
Grand Journal of Urology (GJU) aims to carry written and visualscientific urology studies to academic platforms and to
make significant contributions to the science of urology. Our journal has been abstracted/indexed in Tubitak Ulakbim TR
Index, EBSCOhost, J-Gate, SciLit, ResearchGate and Google Scholar international databases. As of these achievements,
the Grand Journal of Urology (GJU) has taken its place among the journals indexed by national and international databases.
In this issue of our journal, there are many valuable articles under the subheadings of Andrology, Endourology, General
Urology, Reconstructive Urology, Urolithiasis and Urologic Oncology. I hope that these carefully prepared articles will
make important contributions to valuable readers, researchers and the urology literature.
On this occasion, I would like to express my heartfelt gratitude to our authors who have contributed to our journal with
their articles, to our reviewers who have meticulously evaluate the articles.
Respectfully yours
May 2026
Assoc. Prof. Ekrem GUNER, MD
Editor-in-Chief
Rıdvan Kayar, Kemal Kayar, İlker Artuk, et al.
Hematospermia (HS), characterized by the presence of blood
in semen, is a relatively rare clinical finding that often causes
significant concern for patients despite its typically benign nature.
While a specific etiology is frequently not identified, underlying
infectious, inflammatory, or—less commonly—malignant
conditions may occasionally be responsible []. Although HS is
often a self-limiting condition, further evaluation may be warranted
based on factors such as the patient"s age, recurrence of
symptoms, and the presence of accompanying findings. Diagnostic
assessments may include urinalysis, urine or semen cultures,
digital rectal examination, prostate-specific antigen (PSA)
testing, transrectal ultrasonography, and pelvic magnetic resonance
imaging in selected cases []. The 2025 guidelines of the
European Association of Urology (EAU) on Male Sexual and
Reproductive Health propose a structured diagnostic pathway
for HS, recommending further evaluation particularly in men
over 40 years of age, in cases of recurrent episodes, or when
accompanied by additional urological symptoms [].
Nevertheless, despite the presence of evidence-based guidelines,
diagnostic and therapeutic approaches to HS remain highly
variable in routine clinical settings. In Türkiye, factors such
as differences in clinical experience, institutional protocols,
and educational backgrounds may contribute to this variability
among urologists. However, there is a lack of data on how HS is
actually evaluated and managed in everyday urological practice
across the country. This study aimed to assess the diagnostic and
treatment approaches toward HS among practicing urologists
and residents in Türkiye through a pilot cross-sectional survey
involving participants from diverse institutions.
Burak Köseoğlu, Mücahit Çaviş
Kidney cysts are one of the most common benign acquired
kidney lesions []. Autopsy studies show that about half of patients
aged 50 and older have a kidney cyst []. Population-based
studies indicate that simple renal cysts occur in approximately
7-10% of the general population, and their prevalence increases
with age, reaching up to 30% in individuals over 50 years [].
Kidney cysts are classified according to imaging methods as
simple kidney cysts and complex kidney cysts []. Kidney cysts
are usually asymptomatic and are diagnosed incidentally.
Treatment is not necessary unless the cyst becomes infected or
grows and causes symptoms. Treatment options for symptomatic
benign renal cysts are cyst aspiration, surgical resection and
sclerotherapy []. Although there is no evidence that any of the
options is superior to the other; sclerotherapy and aspiration are
associated with a higher incidence of cyst recurrence.
The internet, which started to be used in the second half of
the twentieth century, has become the main source of obtaining
information today. Especially social media platforms are the
resources that patients and health professionals often use to access
health information. Video is an effective way to demonstrate
some content that cannot be easily explained in text form.
YouTube (Google LLC, CA, USA), one of the most widely used
social media platforms where users upload billions of hours of
videos every day, was launched in 2005 []. YouTube can serve
as educational tools for healthcare professionals, patients and
their caregivers. However, videos are uploaded to this platform
without any quality control and the information provided may be
incorrect and misleading []. For this reason healthcare providers
are concerned about the quality and standard of information on
YouTube []. As a result, it is necessary to obtain information
from sources of adequate quality and standard by evaluating the
quality and standards of the content on YouTube.
Until this time, numerous studies in various medical fields
have examined the quality and accuracy of YouTube videos,
reporting that the content may range from highly informative to
biased or misleading [-]. Within urology, the most popular
topics seem to be urooncology and andrology [-]. Kidney
cysts, which are usually detected incidentally in patients
undergoing imaging for another reason, are a fairly common
urological condition. Owing to their high prevalence, kidney
cysts are also among the frequently searched conditions on the
internet and social media platforms.
Despite the growing popularity of video-based medical
learning, no prior studies have systematically assessed the
quality of YouTube content on kidney cysts.
We hypothesized that YouTube videos related to kidney cysts
would vary widely in quality and reliability, with a significant
proportion lacking essential, accurate, or evidence-based
information. Therefore, the aim of this study was to evaluate
the content, reliability, and quality of kidney cyst-related videos
available on YouTube.
Gökhan Şahin, Arif Kol, Mustafa Tıpırdamaz, et al.
Bladder cancer is the tenth most common malignancy
worldwide and is associated with a high mortality rate if left
untreated []. It is classified into two major categories: nonmuscle
invasive bladder cancer (NMIBC) and muscle-invasive
bladder cancer (MIBC), with NMIBC accounting for the majority
of cases. NMIBC includes mucosa-limited (pTa), lamina
propria-invasive (pT1), and carcinoma in situ (CIS) stages. If
untreated, approximately 50% of NMIBC cases progress to
MIBC. Additionally, the recurrence rate after treatment remains
high, ranging from 70% to 80% [].
Ultrasonography (USG) and computed tomography (CT)
urography are commonly used for the diagnosis of urinary tract
pathologies. While USG is useful for detecting intra-bladder
tumors, assessing hydronephrosis, and characterizing renal tumors,
it is limited in its ability to identify upper urinary tract tumors [].
CT urography is typically performed in three phases: the noncontrast
phase, the nephrographic phase (with an 80–120 second
delay), and the excretory phase (with a 10–15 minute delay) []. It
is highly sensitive for detecting renal masses and identifying filling
defects within the urinary collecting system [,].
Neoplastic tissues are known to exhibit high vascularization
to support proliferation and maintain viability []. The angiogenic
activity of malignant tissues is believed to have prognostic
significance. Studies assessing the vascularization of bladder and
renal pelvis tumors have demonstrated an association between
tumoral vascularization and tumor grade, stage, and prognosis
[8,9]. In these studies, vascularization was typically evaluated
using immunohistochemical staining, vessel quantification, or
contrast-enhanced imaging techniques [-].
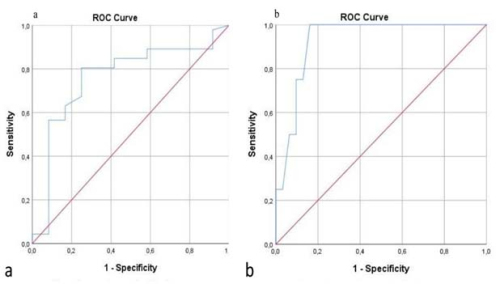
Contrast enhancement techniques have emerged as valuable
methods for assessing bladder cancer, offering insights into tumor
aggressiveness and aiding in staging and grading. Contrastenhanced
ultrasound (CEUS) has been explored for its diagnostic
accuracy in differentiating between muscle-invasive and nonmuscle-
invasive bladder cancer, offering a cost-effective and
safe imaging alternative [,]. Contrast enhancement observed
in CT urography has been demonstrated to correlate with tumor
vascularization and histological grade [].
This study aimed to assess the prognostic significance of
contrast enhancement in CT urography for bladder cancer.
Kenan Yalçın, Vildan Kölükçü
Circumcision is one of the oldest and most widely practiced
surgical procedures worldwide, performed for religious, cultural,
or medical reasons. It is estimated that approximately 30–33%
of men aged 15 years and older have undergone circumcision
globally []. The procedure involves the surgical removal of
the foreskin covering the glans penis. Despite being commonly
performed, circumcision should not be regarded as a simple
or minor intervention. The accurate identification of excision
margins, strict adherence to antiseptic principles, and the
provision of adequate analgesia and anesthesia are all essential
for ensuring safe and optimal surgical outcomes [].
The optimal timing for circumcision remains of topic of
ongoing debate in both clinical and sociocultural contexts [].
Similarly, there is no universally accepted or standardized
protocol regarding the choice of anesthesia []. In Freudian
psychoanalytic theory the so-called "phallic stage", between
three and six years of age, represents a critical developmental
period during which children begin to form their gender identity,
establish body awareness, and internalize attitudes toward
sexuality and the body []. Although there is a lack of high-level
evidence from large-scale studies or meta-analyses, a significant
proportion of healthcare professionals express concern about
performing circumcision during this stage due to its potential
association with castration anxiety, body image disturbances, and
adverse psychosexual outcomes [,]. Nevertheless, circumcision
during this developmental period remains common in many
cultures, particularly when performed under local anesthesia for
religious or traditional reasons. In pediatric patients within this
age group, the procedure may trigger feelings of fear and anxiety,
which could potentially contribute to long-term psychological
consequences [,].
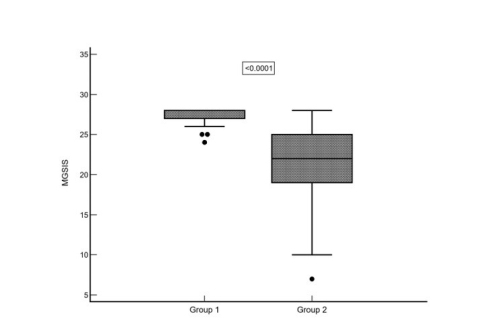
To the best of our knowledge, this is the first study in the
English-language literature to examine the long-term effect of
the anesthesia type administered during circumcision in the
phallic stage on adult male genital self-image.
Süleyman Şahin, Metin Savun, Çağrı Şevik, et al.
Ureteral injuries, although relatively uncommon, represent
a serious surgical complication that can result in significant
morbidity, including ureteral stricture, hydronephrosis, and loss
of renal function if not promptly diagnosed and managed. The
vast majority are iatrogenic in nature, with the distal third of
the ureter being particularly vulnerable during pelvic procedures
such as gynecological, colorectal, and urological surgeries [–].
Definitive management of distal ureteral injuries typically
requires surgical reconstruction to restore urinary continuity
and preserve renal function. Ureteroneocystostomy is the most
widely accepted approach, with several techniques described,
including the Politano–Leadbetter and the extravesical Lich–
Gregoir methods []. The Lich–Gregoir technique, originally
developed for anti-reflux ureteral reimplantation, has become
popular due to its relative technical simplicity, shorter operative
time, and low complication profile [].
Over time, several modifications of the Lich–Gregoir technique
have been introduced to optimize outcomes, especially in complex
or reoperative settings. The extravesical approach minimizes
bladder dissection and avoids extensive intravesical manipulation,
which can be advantageous in patients with iatrogenic injuries
after major pelvic surgery. However, the evidence specifically
addressing the role of the modified Lich–Gregoir technique in
adult iatrogenic distal ureteral injuries remains scarce. Most
previous reports have either pooled various etiologies or focused
primarily on pediatric or reflux populations [,].
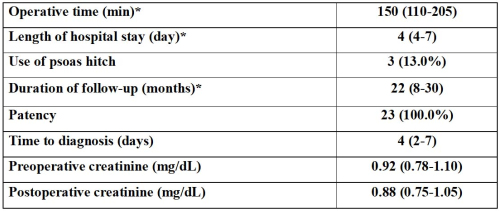
The objective of this study was to assess the surgical and
functional outcomes of repairing iatrogenic injuries to the distal
ureter using the modified Lich–Gregoir ureteroneocystostomy
technique, with a focus on perioperative factors, complication
rates, and long-term functional outcomes.
İbrahim Can Aykanat, Buğra Cidani, Muhammed Çakır, et al.
Peyronie"s disease is a condition characterized by the
formation of fibrotic plaques within the tunica albuginea of the
penis, leading to penile curvature, pain, and sexual dysfunction,
thereby significantly impairing male quality of life []. Although
Peyronie"s disease can occur across all age groups, it is most
commonly encountered in middle-aged men. The reported
prevalence of the disease in the literature varies widely, with rates
ranging from 0.3% to 20%. Nevertheless, despite differences in
study methodologies, the most frequently cited prevalence is
approximately 9% [-]. It is well recognized that some patients
avoid seeking medical care due to embarrassment or reluctance,
and even when they do present to healthcare facilities, they often
turn to internet-based resources to obtain additional information
regarding diagnosis and treatment [,].
In recent years, online video-sharing platforms such as
YouTube have become easily accessible sources of health-related
information for patients. Indeed, in daily urological practice, it is
frequently observed that patients actively use YouTube to acquire
supplementary information about their medical conditions
[-]. However, the quality of content available on YouTube
is not always adequate, and the largely unregulated nature of
the platform may facilitate the dissemination of misleading or
inaccurate information.
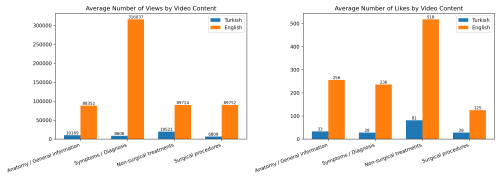
Although studies evaluating the content quality and reliability
of English-language YouTube videos related to Peyronie"s
disease are available in the literature, there is currently no study
focusing on Turkish-language content []. Therefore, the aim
of the present study was to comparatively evaluate Turkish and
English YouTube videos related to Peyronie's disease in terms
of content, quality, and reliability.
Gaëtan Devos, Xander De Troyer, Carl Van Haute
Ureteroceles are defined as cystic dilatations of the terminal
ureter within the bladder and result from a congenital defect
in ureteral embryogenesis []. They are classically diagnosed
in pediatric populations, often associated with duplicated
collecting systems and extravesical localisation (ectopic in the
bladder neck or urethra). In contrast, adult ureteroceles are rare,
typically intravesical (or orthotopic), and frequently discovered
incidentally [,].
Clinical presentation in adults ranges from asymptomatic
findings to recurrent urinary tract infections, urolithiasis,
hematuria, or obstruction. Prolapse of a ureterocele through the
urethra has been described only sporadically in the literature [].
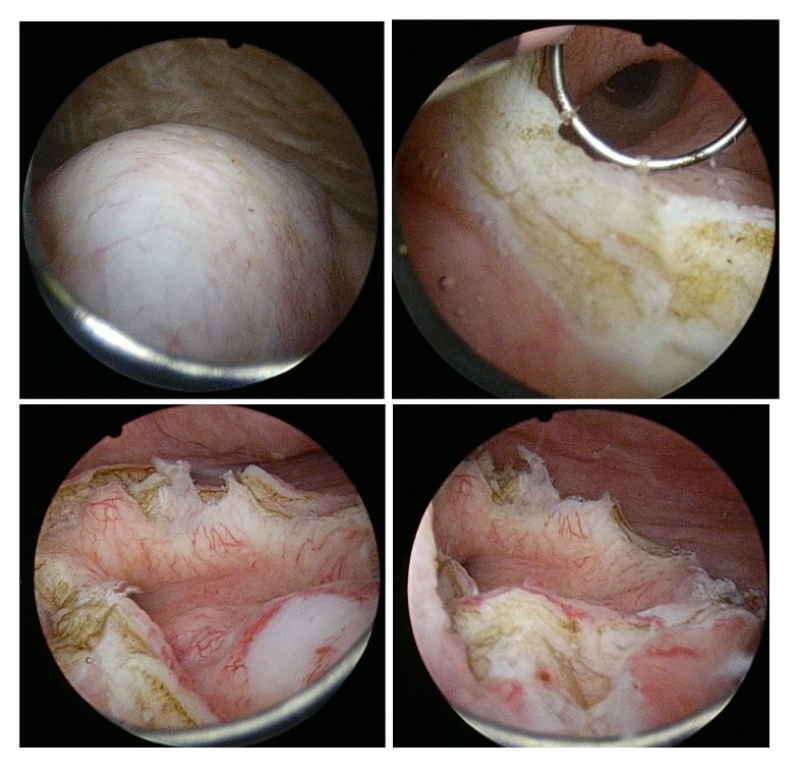
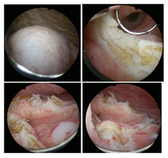
Management strategies include observation, endoscopic
incision or resection, and open or minimally invasive ureteral
reimplantation []. However, due to the rarity of this condition
in adults, no consensus guidelines exist. We present a rare case
of a giant prolapsed ureterocele in an adult woman treated
successfully with endoscopic deroofing, and we review the
relevant literature.
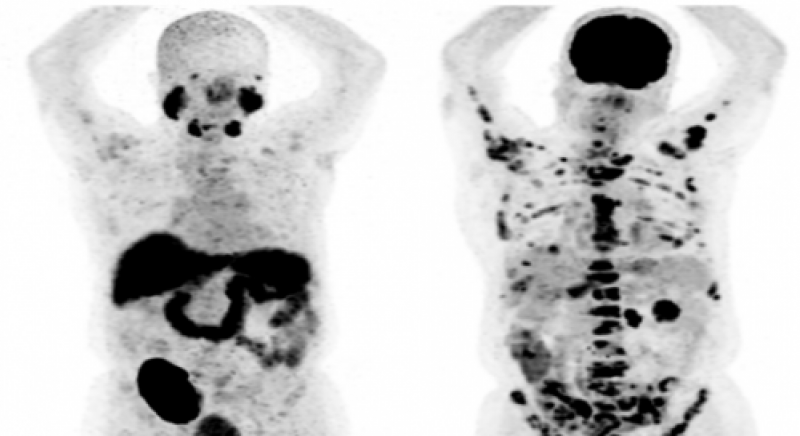
Ryoya Oka, Atsushi Okita

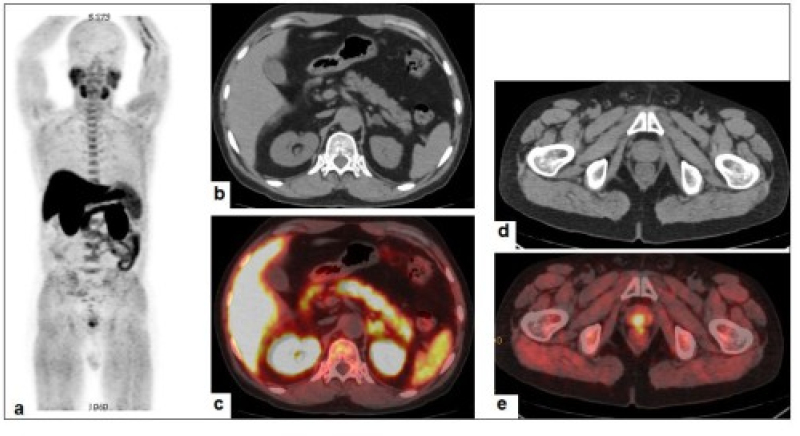
A 78-year-old male patient presented to our hospital with
a slowly enlarging, painless right inguinal mass that had been
present for 15 years. On physical examination, a non-tender right
scrotal mass was palpable. Computed tomography revealed a
12-cm encapsulated cystic lesion containing a calculus (Figure
1). Blood tests showed a mildly elevated C-reactive protein
(CRP) level of 0.74 mg/dL (reference range: < 0.14 mg/dL).
Based on these findings, a diagnosis of right scrotal hydrocele
was made, and the patient underwent right orchiectomy with
hydrocelectomy. Intraoperative findings indicated that the mass
was located in the scrotum and extended toward the external
inguinal ring. Orchiectomy was selected because the hydrocele
was firmly adherent to the testis, with chronic inflammation
and fibrosis, making safe separation technically unfeasible.
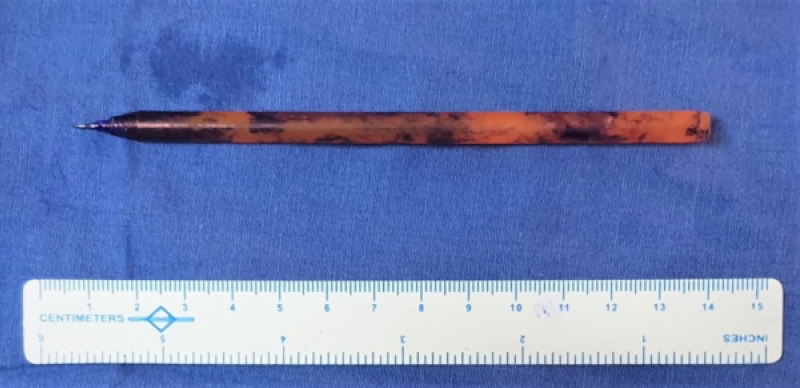
The resected specimen contained turbid fluid, a calculus, and a
markedly thickened, inflamed, and partially necrotic cyst wall
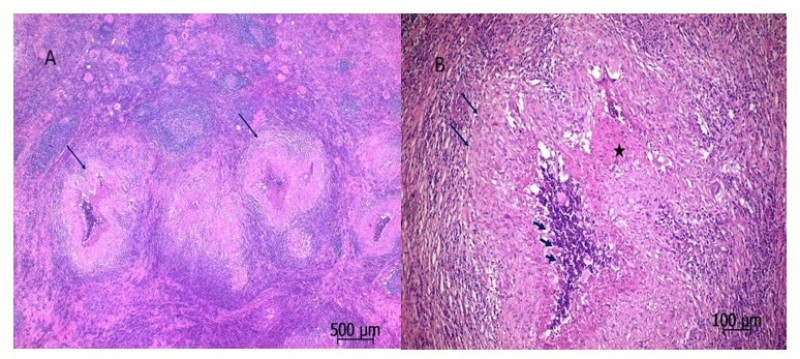
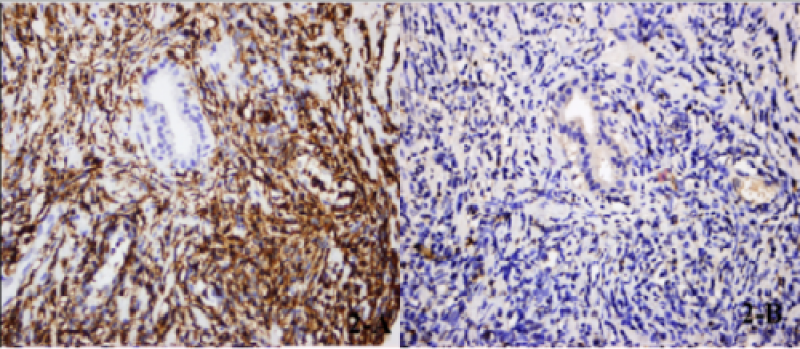
(Figure 2). Histopathological examination revealed diffuse
thickening of the tunica vaginalis with dense lymphoplasmacytic
infiltration and characteristic storiform fibrosis (Figure 3A). The
testis itself was markedly atrophic, and the seminiferous tubules
showed diffuse atrophy with thickened basement membranes and hyalinization. The hydrocele was not located within the testicular
parenchyma. Immunohistochemical staining demonstrated
27-48 Immunoglobulin G4 (IgG4)-positive plasma cells per
high-power field (HPF) and an IgG4-positive/IgG-positive
plasma cell ratio of 25-55% (Figure 3B). Given the patient's
long-standing, slowly enlarging inguinal mass without prior
hospital visits, and the marked chronic inflammatory changes
observed intraoperatively and pathologically, the exact origin
and progression from the inguinal area cannot be determined.
Figure 1. Computed tomography image. Computed
tomography scan showing a 12-cm encapsulated cystic
lesion with a calcified nodule in the right inguinal region
Figure 2. Gross appearance of the resected specimen showing
a thickened, inflamed, and focally necrotic cyst wall
Figure 3. A- Histopathological examination revealing
lymphoplasmacytic infiltration and storiform fibrosis (H&E
×100), B- Immunohistochemical stain highlighting numerous
IgG4 positive plasma cells (×400)
Serum IgG4 was within normal limits, and no involvement
of other organs was observed. According to the 2019
American College of Rheumatology/European League Against
Rheumatism (ACR/EULAR) classification criteria for IgG4-
related disease [], a diagnosis of IgG4-related disease (IgG4-
RD) was established. The postoperative course was uneventful,
and the patient remains well on follow-up.
IgG4-RD is a recently recognized, immune-mediated
fibroinflammatory disorder characterized by tissue infiltration
with IgG4-positive plasma cells, lymphoplasmacytic
inflammation, storiform fibrosis, and frequently obliterative
phlebitis []. It can involve multiple organs, most commonly the pancreas, salivary glands, and lacrimal glands, resulting in
clinical entities such as autoimmune pancreatitis, sialadenitis,
and dacryoadenitis. Corticosteroid therapy is considered the
first-line treatment, although no randomized controlled trials
have been conducted to date. In the present case, systemic
therapy was not initiated because serum IgG4 was normal and
there was no evidence of extra-scrotal disease.
Reports of IgG4-RD involving the male reproductive
system are rare, with only a few testicular cases described in
the literature. To our knowledge, presentation as chronic scrotal
hydrocele represents an exceptionally uncommon manifestation.
This case underscores the importance of considering IgG4-RD
in the differential diagnosis of long-standing scrotal masses,
particularly when histological features are suggestive. Increased
awareness of this entity may facilitate accurate diagnosis,
appropriate management, and a deeper understanding of its
diverse clinical spectrum.
Ethics Committee Approval: N/A
Informed Consent: An informed consent was obtained from
the patient.
Publication: The results of the study were not published in full
or in part in form of abstracts.
Peer-review: Externally peer-reviewed.
Conflict of Interest: The authors declare that they have no
conflicts of interest.
Financial Disclosure: The authors declare that this study
received no financial support.