Ekrem GUNER

Dear colleagues,
I am honored to share with you the third issue of 2023 (volume 3, issue 3) of the Grand Journal of Urology (Grand J Urol) with the contributions of many respected researchers and authors.
Grand Journal of Urology (GJU) aims to carry written and visual scientific urology studies to academic platforms and to make significant contributions to the science of urology.
Our journal has been abstracted/indexed in Tubitak Ulakbim TR Index, DOAJ, EBSCOhost, J-Gate, Index Copernicus International, EuroPub, SciLit, ResearchGate, ScienceGate and Google Scholar international databases. As of these achievements, the Grand Journal of Urology (GJU) has taken its place among the journals indexed by national and international databases.
In this issue of our journal, there are many valuable articles under the subheadings of General Urology, Neurourology, Urolithiasis and Urological Oncology. I hope that these carefully prepared articles will make important contributions to valuable readers, researchers and the urology literature.
On this occasion, I would like to express my heartfelt gratitude to our authors who have contributed to our journal with their articles, to our reviewers who have meticulously evaluate the articles.
Respectfully yours
January 2024
Assoc. Prof. Ekrem GUNER, MD
Editor-in-Chief
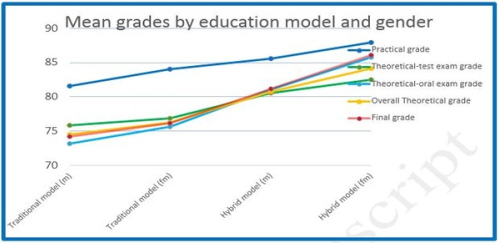
Erdem Akbay, Erim Erdem, Selahittin Cayan, et al.
Advances in telecommunication technology such as mobile
internet devices have changed medical educational practices in
academic centers. Today, the biggest benefit of the use of mobile
phones and laptops for education is that they provide a great deal
of freedom regarding the time and place at which information is
obtained []. In recent years, the transfer of educational programs
to virtual platforms has begun to take its place in medical
education. Applications used in other fields of education have
become important tools when used for medical education [].
The development of instant messaging applications, especially
on mobile phones, has gained popularity among healthcare
professionals and medical students.
Traditional medicine education continues to be the cornerstone
of many educational institutions in the world. In addition to
traditional education, the use of mobile devices will be essential for
the education and exams of medical students, interns, and medical
residents [-]. There is limited information in the literature about
the place of hybrid models in urology. In this study, we have
compared training success rates between traditional and hybrid
model of education among 4th-year medical students rotating in
urology clinics of a university hospital.
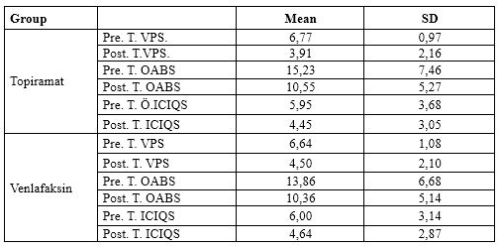
Sinan Eliacık, Aykut Baser, Funda Uysal Tan
Chronic migraine (CM) is a disease that negatively affects
the quality of life of individuals, and it is more common in
women, it affects approximately 12% of the general population.
Similarly, overactive bladder (OAB), the most common subtype
of urinary incontinence, has also an adverse effect on life quality.
Unfortunately, most women hardly reveal their complaints,
living with the course despite worsening of OAB symptoms.
Altman et. al. have documented the association between OAB
and various somatic disorders []. The comorbidity between
CM and OAB was also supported by other studies, however,
both disorders have complex multifactorial etiopathogenesis
affected by both environmental and genetic factors []. Thus, the
physiopathological basis of the possible association between CM
and OAB remains obscure. Based on the study in which we found
an association between CM and OAB; suspecting a common
etiopathogenesis behind the comorbidity, we aimed to determine
whether migraine prophylaxis would affect the symptom severity
of OAB []. Thus, we evaluated the changes in OAB symptoms
in patients given migraine prophylaxis treatment.
Kenan Yalcin, Erim Ersoy
With the higher prevalence of surgical interventions that
reduce renal blood flow such as transplantation, trauma,
anatrophic nephrolithotomy, nephron-sparing surgery, and
renal artery surgery ischemia-reperfusion injury has been more
frequently cited in the literature. In ischemia, oxygen required
to maintain aerobic metabolism is not supplied to the living
tissue. Recovery of normal blood flow after a period of ischemia
is called reperfusion. Since the self-control of the metabolism
of the oxygen entering the atmosphere with reperfusion of
the organ that remains ischemic for a while deteriorates,
free oxygen radicals (FORs) with their toxic effects become
manifest and cause ischemia-reperfusion injury in the tissue.
Along with emerging FORs, activation of various proteases and
phospholipase A2 by calcium entering the cell during ischemia
is also a response to ischemia-reperfusion injury [-].
The response that organs give to experimental ischemiareperfusion
injury was very well specified in the rats and
rats were preferred as experimental animals in most of the
literature studies [-]. During ischemia, the tissue is damaged
by asphyxiation and when the normal blood flow is retrieved,
tissue damage aggravates greatly as a result of a series of events
caused by the oxygen entering the atmosphere [,].
Mitochondrial electron transport chain reactions, inhibition
of arachidonic acid metabolites, increase in intracellular calcium
levels, xanthine oxidase system, iron ion, etc. involve in the
production of FORs which induce ischemia-reperfusion injury
in the kidney tissue. These factors affect each other sequentially
and disrupt cell functions, increase membrane destruction, and
result in the production of endogenous toxins [-].
The only way of treatment in ischemic kidneys is to increase the
renal blood flow through reperfusion. Yet in that case reperfusion
damage inevitably occurs. In such a case, since the increase of
blood supply is inevitable, it is necessary to look for solutions
to prevent reperfusion damage. Many agents such as vitamin E,
melatonin, phospholipase type 3 enzyme inhibitors (amrinone,
olprinone), adenosine, n-acetyl cysteine, nitric oxide (NO),
calcium channel blockers, mycophenolate mofetil have been used
in order to prevent or alleviate renal ischemia-reperfusion injury
associated with various etiologic factors [,].
Diosmin-hesperidin is produced by the purification of
flavonoid extracts of a plant found in the nature. Daflon is a
phlebotonic and vasculoprotector agent that is comprised of
90% diosmin and 10% hesperidin. Hesperidin reinforces the
activity of diosmin, improves wound recovery by acting against
inflammatory mediators and protects microcirculation via
decreasing blood viscosity [].
Diosmin-hesperidin has also shown anti-inflammatory effects
through many mechanisms of action in our study. Many studies
have been conducted on significant ischemia-reperfusion injury
preventing effects of diosmin-hesperidin in multiple organs such
as heart, brain muscle tissue, and peritoneum [,].
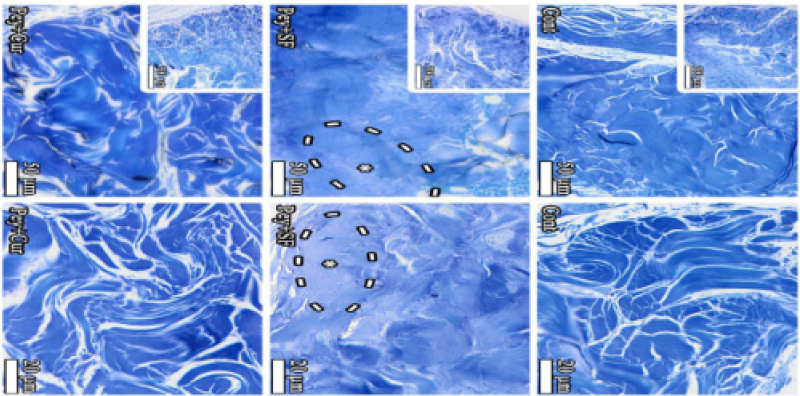
Diosmin-hesperidin is an important antioxidant drug
combination. Leukocyte aggregation is important in ischemiareperfusion
injury and damage can be prevented with diosminhesperidin
at daily oral doses of 500 mg. Also, this drug
combination reduces the amount of H2O2 released from
leukocytes by suppressing activity of myeloperoxidase (MPO). A decrease in the MPO activity can explain the decrease in
H2O2 in the group that received diosmin-hesperidin at doses
protecting against oxidative stress associated with glutathione
(GSH). Diosmin-hesperidin given at doses protecting against
oxidative stress associated with GSH guards the escape of
macromolecules from the microvascular structures. According to
histopathological data, diosmin-hesperidin prevents infiltration
of leukocytes into the perivascular area. Although it does not
totally prevent leukocyte infiltration, a significant reduction in
leukocyte accumulation in the perivascular area in the kidney
was observed [].
We have aimed to experimentally investigate the activity of
diosmin-hesperidin, which acts against inflammatory mediators
in ischemia-reperfusion injury and protects microcirculation
by decreasing blood viscosity in cases with renal ischemiareperfusion
injury.
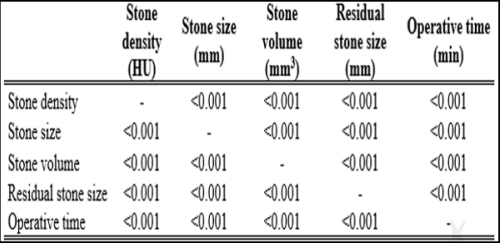
Muhittin Atar, Abdullah Turan, Ali Haydar Yilmaz, et al.
Urinary system stone disease is one of the oldest diseases
affecting human health. The prevalence rate of stone disease
varies between 1 and 20%, depending on climate, ethnic
characteristics, genetics, and dietary habits. Among individuals
with stone disease experiencing at least one episode in
their lifetime, the recurrence rate has been reported to be
approximately 50% []. The prevalence of stone disease is
3-11% in Europe; however, in regions with hot climates, such as
Africa and the Middle East, it can reach 20% [,]. In Türkiye,
this rate was found to be 14.8% according to a study conducted
by Akınci et al. [].
Non-contrast computed tomography (CT) has now replaced
urography as the gold standard due to its high sensitivity and
accuracy in diagnosing urolithiasis and the incorporation of
new techniques to reduce radiation doses [,]. In addition
to the diagnosis of urolithiasis, CT also provides important
information concerning stone location, stone density, stone
size, stone volume, stone-to-skin distance, hydronephrosis, and
perinephric stranding. Stone density is determined by measuring
the Hounsfield unit (HU) of the stone on CT. Through these
measurements, the hardness, composition, heterogeneity, or
homogeneity of the stone can be calculated. This information
is important for clinicians to determine the fragility of the stone
[-]. Evaluation of stone density has been integrated into daily
medical practice to decide on the best treatment option for urinary
tract stone disease. It has been suggested that HU affects the
success of lithotripsy in treatment methods such as extracorporeal
shock wave lithotripsy (ESWL), ureterorenoscopy (URS), and
percutaneous nephrolithotomy (PCNL) [-].
We hypothesized that stone density would affect the duration
of lithotripsy performed with a Holmium laser as well as the
postoperative stone-free outcome. Thus, large-volume kidney
and ureteral stones with low stone density can be treated with URS
and RIRS, and stone density can be an important determinant in
case selection. In this study, we aimed to investigate the effect of
stone density on the success of URS and RIRS in the treatment
of kidney and ureteral stones.
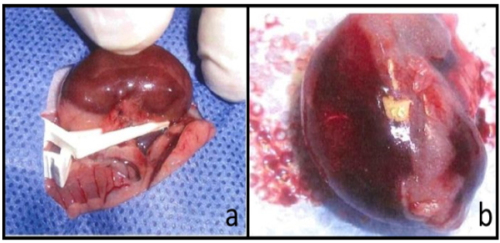
Kenan Yalcin
Wilms tumor (WT) is the most common renal tumor in
childhood period, affecting one in 10,000 children [–]. It is
mostly seen between the ages of 2-4. WT is an embriological
tumor that classicaly shows a triphasic histological complex
structure originating from blastem, epithelial and stroma
components. Besides that it may also includes cartilage, osteoid
and neuronal elements [].
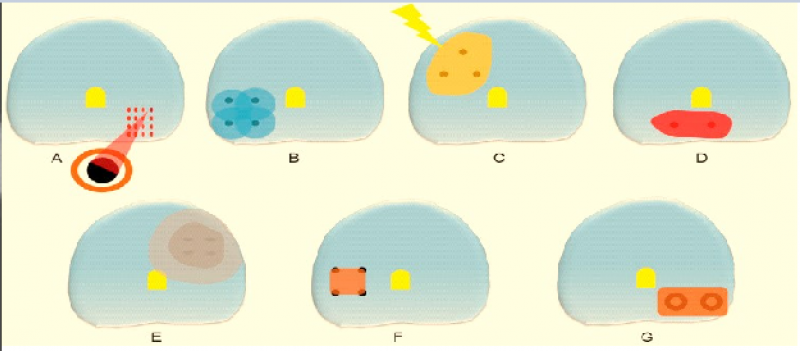
The WT treatment is implemented with two distinctive
methods: The Europe"s International Society of Pediatric
Oncology (SIOP) method which adopts the principle of
initiating chemotherapy (CT) without tissue diagnosis and
then surgical application and North America"s National
Wilms Tumor Study (NWTS), now known as the Children"s
Oncology Group method (COG) which carries out a treatment
plan with tissue diagnosis. Primarly providing CT contributes
to preventation of phase escalation due to tumor cells being
shed during surgery and surgical complications that may occur
in the presence of large-sized or thrombus but besides that
has a disadvantage of providing unnecessary CT to the cases
diagnosed histopathologically other than WT. In NWTS/COG
method, although tissue diagnosis is the main criterion, the
principle of providing CT first is adopted in very large tumors,
bilateral cases and the presence of thrombus extending into the
IVC or atrium. However, the most important factor determining
the prognosis in both methods is the phase of tumor, whether
it contains anaplasia and the positivity of biological indicators
such as 1p, 16q LOH veya 11p15q LOH [,,].
Surgery is one of the key factors in WT treatment.
Transperitoneal radical nephrectomy is standard operation for
unilateral WTs. Nephron sparing surgery is suggested to be
implemented in selected patient cases with single kidneys or
bilateral WT. In this case report, a patient who diagnosed with
Wilms tumor in right kidney at the age of 4 and underwent
partial nephrectomy which is rarely implemented or suggested
to be implemented in selected cases is represented.
Somanatha Sharma, Kiritha Ranjani Ac, Sethu Ram Sharma
Chest wall malignancies are considered rare, constituting
approximately 1% of all malignancies. These malignancies
may originate primarily from bone or soft tissue, result from the
infiltration of adjacent organ malignancies, or occur secondary
to distant metastasis, with the latter being the predominant cause
[]. Prostate cancer, ranking as the second most diagnosed cancer
in men and the fourth most common overall, typically exhibits
metastasis to various sites, including bone, lymph nodes, lung,
bladder, liver, and adrenal glands [].
While the literature reports prostatic metastases to almost
every organ in the body, involvement of the sternum is
notably infrequent in prostate cancer cases []. Within sternum
involvement, osteosclerotic metastasis have been documented,
yet osteolytic metastasis in the sternum due to prostate cancer
remains an exceedingly rare occurrence, lacking documented
cases in medical literature [].
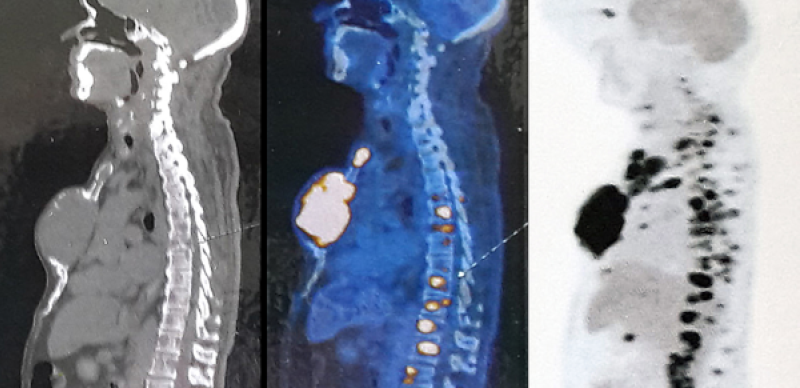
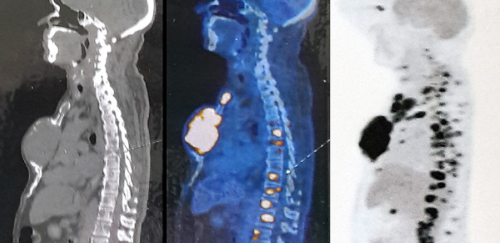
This article presents a noteworthy case of metastatic prostate
cancer, wherein the clinical presentation manifested as a
sizable sternal mass. Further evaluation revealed an expansile
osteolytic sternal body metastasis in a 75-year-old gentleman.
The peculiarity of this manifestation, along with its diagnostic
and therapeutic challenges, underscores the need for a detailed
examination of such atypical cases.
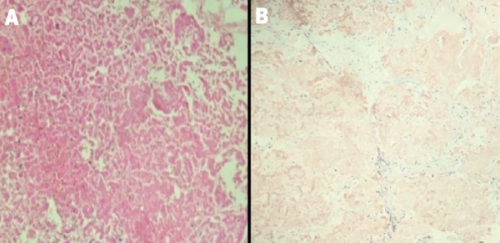
Saurabh Kumar Negi, Sandip Desai, Gaurav Faujdar, et al.
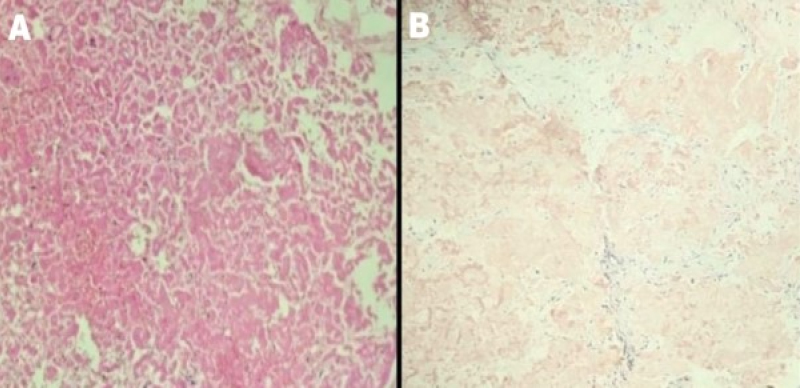
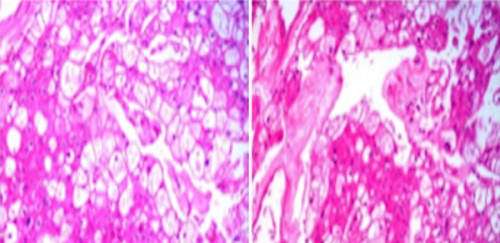
Amyloidosis is a rare disease characterized by deposition
of extracellular, hyaline and proteinaceous material in various
organs. Amyloidosis can be primary, secondary, and hereditary.
Localized amyloidosis of the urinary bladder is rare easily
confused with an infiltrating tumor on imaging and cystoscopy
[]. Accurate diagnosis depends on biopsy showing negative
malignant cells and presence of amyloid fibrils on cong red
staining.